News Center
Vocal cord granulomas diagnosed on reviewing videolaryngoscopy images
A 1-year-old girl with trisomy 21 was admitted to the paedi-atric intensive care unit (PICU) with respiratory distressrequiring endotracheal intubation and mechanical ventilation.She required a prolonged period of intubation despite multipleattempts to extubate.
One re-intubation towards the end of her PICU admission was performed using a Vimed video laryngoscope (Vimac, Hebei Vimed Medical Device Company). When reviewing footage recorded on the video laryngoscope, bilateral vocal cord lesions(figure 1) were noted. The patient was discussed with the ear,nose, throat (ENT) surgeon who was able to view the recorded images and diagnose the lesions as vocal cord granulomas.
Vocal cord granulomas are a recognised complication of intu-bation. Contact ulcers to the larynx can occur which heal byre-epithelialisation which can sometimes result in granulomaformation. 1Post extubation stridor was not an issue in this case. Reviewingthe clinical history and the videolaryngoscope images enabled
the ENT surgeon to reassure us that the granulomas were likelyto be an incidental finding and not a contributing factor toextubation failure. This negated the need for further invasiveprocedures.
Treatment options depend on the underlying cause and canbe conservative or surgical. In this case the initial treatment planwas extubation at the earliest opportunity. 2Studies have demonstrated that video laryngoscopes generallyprovide a better view of the glottis and can achieve a highersuccess rate of tracheal intubation in patients with difficultairways when compared with direct laryngoscopy. 3 It has alsobeen proposed that they are potentially useful as a teaching tool. 4This case highlights another advantage of videolaryngoscopy.
The ability to record and retrospectively review the intubationimages allows an opportunity to diagnose coexisting disease. Inthis case we noted vocal cord granulomas. We have also inci-dentally noted tonsillitis on a number of occasions when usingvideolaryngoscopy in the PICU.
Alison Price, 1 Sara Lawson, 2 Christopher Flannigan 1
1 PICU, Royal Belfast Hospital for Sick Children, Belfast, UK
2 Neonatal Intensive Care Unit, Royal Jubilee Maternity Hospital, Belfast, UK
Correspondence to Dr Alison Price, PICU, Royal Belfast Hospital for Sick Children,Belfast BT12 6BA, UK; aprice07@ qub. ac. uk
Contributors AP and SL wrote the article. CF reviewed the article prior tosubmission.
Competing interests None declared.
Patient consent Parental/guardian consent obtained.
Provenance and peer review Not commissioned; externally peer reviewed.
© Author(s) (or their employer(s)) 2019. No commercial re-use. See rights andpermissions. Published by BMJ.
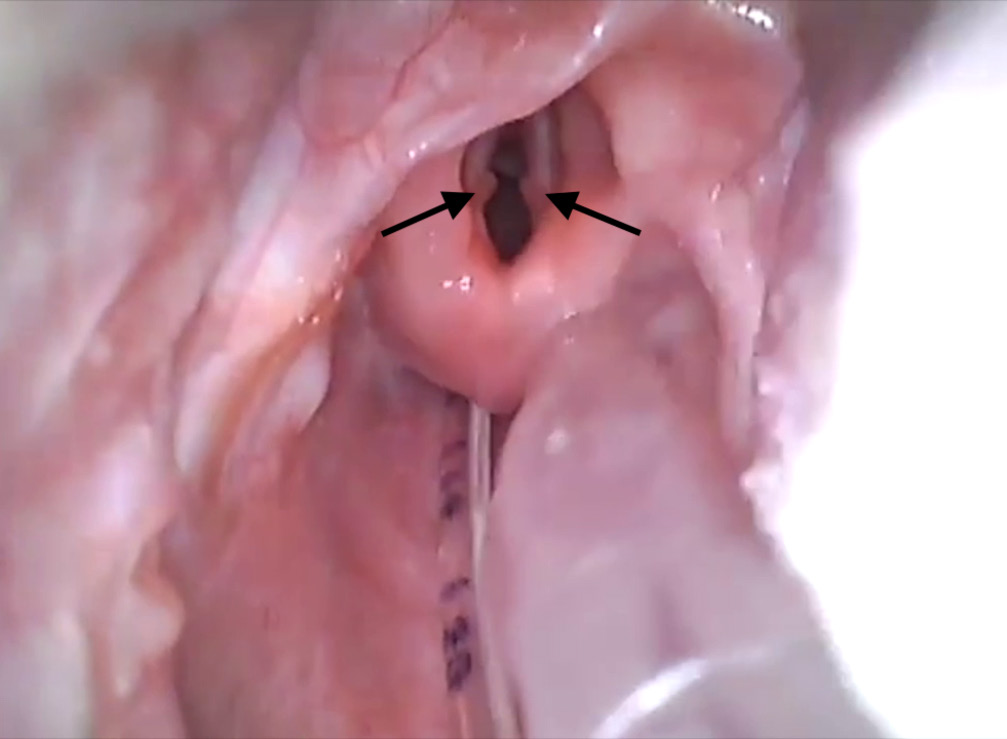
Figure 1 Bilateral vocal cord granulomas noted during endotracheal intubation using Vimac video laryngoscope.
To cite Price A, Lawson S, Flannigan C. Arch Dis Child Epub ahead of print: [please include Day Month Year]. doi:10.1136/archdischild-2018-316160
Accepted 8 December 2018
Arch Dis Child 2019;0:1. doi:10.1136/archdischild-2018-316160
RefeRences
1. Evans D, McGlashan J, Norris A. Iatrogenic airway injury. BJA Educ 2015;15:184–9.
2. Karkos PD, George M, Van Der Veen J, et al. Vocal process granulomas: a systematic review of treatment. Ann Otol Rhinol Laryngol 2014;123:314–20.
3. Asai T. Videolaryngoscopes: do they truly have roles in difficult airways? Anesthesiology 2012;116:515–7.
4. Lingappan K, Arnold JL, Fernandes CJ, et al. Videolaryngoscopy versus direclaryngoscopy for tracheal intubation in neonates. Cochrane Database Syst Rev2018;137.